That’s right. Tennis Elbow isn’t always caused by playing tennis. In fact, it’s probably more often caused by some other repetitive, strenuous activity.
TENNIS ELBOW, otherwise known as Lateral Epicondylitis, is a very common overuse injury. In practice, I saw it several times a year. The elbow joint is made up of three bones—the humerus, the radius, and the ulna. The upper arm bone, the humerus, is the stabilizing structure to which several muscles and ligaments attach. At the elbow end of the humerus are two bony bumps on the inside and the outside of the elbow. These bumps, or bony prominences, are called epicondyles. The outer bump is the Lateral Epicondyle, and the inside bump is the Medial Epicondyle. Attached to the epicondyles are the tendons of the muscles that rotate the forearm and hand. When the hand rotates so the palm is up, the motion is called Supination. When the forearm rotates the palm downward, the motion is called Pronation. Repeated rotation of the forearm and hand and up and down movement of the wrist, especially against a resistance, cause inflammation of the tendon.
Tennis players get it, but so do plumbers, painters, mechanics, carpenters, cooks, and butchers, and there are a lot more of them than there are tennis players. Overuse of the rotating motion of the forearm and hand against a resistance causes microscopic tears at the point of attachment of the tendon to the lateral epicondyle. The tears result in inflammation at the point of attachment. Inflammation causes pain, tenderness, and sometimes swelling, of the lateral epicondyle.
Patients with tennis elbow have a weak grip and experience pain when turning doorknobs, shaking hands, holding objects in the hand, or using tools. The pain can be bad enough to prevent use of that extremity. I had it one time when the lawn mower starter cord suddenly stopped while I was pulling on it. I had immediate pain that lasted several weeks.
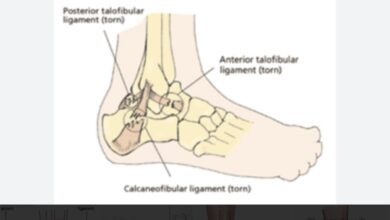
Tennis elbow is truly a tendonitis of the rotating muscle of the forearm, but MRI studies have shown that ligaments of the elbow also tear in a large percentage of patients. Those patients have more pain over a longer duration (average 2.3 years).
The most important point in treatment is to emphasize the tendon needs to be rested, and aggravating activities completely avoided. Ice applications, NSAID’s, a tennis elbow strap, or a shot of cortisone at the site of tenderness, can be helpful.
Surgery is a last resort measure and reserved for those patients who have not responded to non-surgical treatments after 6-12 months, or whose MRI shows a partially or completely torn tendon. “Micro-tears” are not detectable by MRI.
Dr. G’s Opinion: Tennis elbow is an annoying problem that is particularly troublesome if it involves the dominant hand. Using that extremity is painful, and even slight movements will aggravate it. Resting the elbow is a must. Tennis elbow straps help some patients simply by reminding them to rest the elbow, but are often useless. Cortisone shots can be done three months apart if necessary. I had fairly good results with this treatment. Surgery was required in very few of my patients, but those who had it did well and got relief of pain. But recovery took a long time.
My best advice is to stop doing what you’re doing if elbow pain begins. Immediately ice the area for 20 minutes on and 20 minutes off for a couple of hours. Take ibuprofen, 200, 400, or 600 mg. Don’t restart activity until you’re certain the pain has completely subsided. Be very cautious when you do resume activity because pain can easily recur. Good luck with this problem.
References: https://www.orthoinfo.aaos.org/en/diseases—conditions/tennis-elbow-lateral-epicondylitis/
https://www.mayoclinic.org/diseases-conditions/tennis-elbow/
Cha YK,Kim SJ, et al.Magnetic Resonance Imaging of patients with lateral epicondylitis:Relationship between pain and severity of Imaging features in elbow joints. Acta Orthop Traumatol Turc. 2019 Apr 28. pii: S1017-995x(18)30499-1.
Altintes B, Greiner S. Lateral epicondylitis: conservative-operative. Orthopade. 2016 Oct;45(10):870-7.