I just read an article on medscape.com that referred to changes that may be coming in the long-term prevention and treatment of coronary artery disease (CAD). There were two major items discussed that are directly associated with reductions in cardiovascular deaths, non-fatal heart attacks, stent clotting, and major bleeding.
The first of these is a significant change in cholesterol management. The target level for LDL Cholesterol for patients with known CAD and/or diabetes has been lowered from 70 mg/dL to 55 mg/dL. That level can be difficult to reach, but they say reach it using any means at your disposal. Those options include “high intensity statins” such as 20 mg of rosuvastatin or 20-40 mg of atorvastatin plus Zetia, or PCSK9 inhibitors like Repatha or Praluent, or Bempedoic acid. This intense treatment has translated into a reductions in non-fatal heart attacks and coronary bypass procedures.
The other shift comes in the area of coronary artery stents and what is best to prevent them from clotting and blocking blood flow. A 10-year study found that Plavix (clopidogrel) was superior to aspirin for long term maintenance. This has proven to be a good option, again, because of reductions in cardiovascular death, heart attacks, and coronary-related symptoms. Bleeding was less with Plavix vs. aspirin as well. Thus came the recommendation that clopidogrel was better for long term maintenance of “third generation” stents. That’s simple enough, BUT what the heck are “third generation” stents?
I didn’t know what a third generation stent was! And besides that, I didn’t know that there were 3 generations of stents. What are first and second generation stents? What’s the difference between generations? Well, I didn’t know so I went to the favorite website of Larry Page and Sergey Brin, the two founders of GOOGLE.
GOOGLE capsulizes them nicely into 3 generations and even mentions a 4th generation currently being studied. First generation stents were introduced in the late 1980’s. They were developed to keep open an atherosclerotic plaque after angioplasty. Angioplasty breaks open a narrowed artery which would shut down were it not for a stent holding it open. The first stents were “bare metal” made of stainless steel and “durable polymers.” They resembled a Chinese finger trap designed to spring into the open position to keep the artery open. They reduced restenosis (re-closure) from 20% down to 5%, but they required anti-platelet drugs to keep them from clotting.
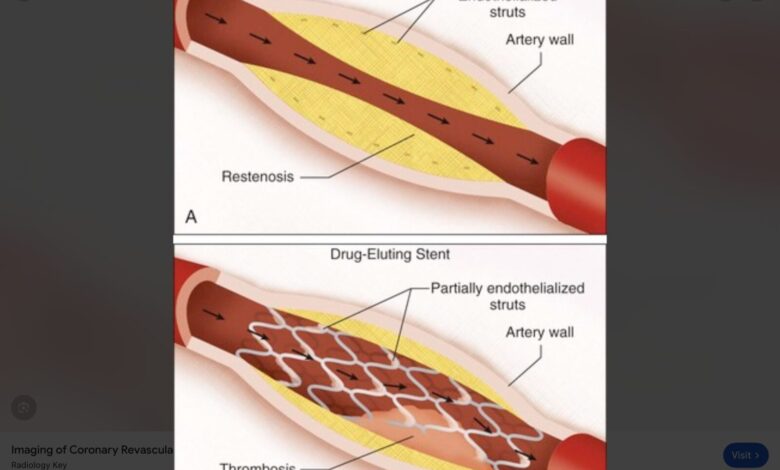
Second generation stents were called “drug-eluting” meaning they were coated with low-dose drugs that prevented clotting and restenosis of the angioplastied vessels. They had thinner metal struts and were made of polymers that withstood inflammation and the clotting it causes. They were safer, more effective, more durable, and easier to put in place. Anti-platelet drugs were still needed but for a shorter time. They were highly regarded until around 2010 when third generation stents were introduced.
Third generation stents were advanced drug-eluting stents with thinner struts, polymers designed to accelerate vessel healing and incorporating into the vessel wall. They were more flexible and easier to place in complex, calcified, small vessel coronary disease. The drugs coating these stents were improved formulations and reduced restenosis even more. They offer improved safety and utility over their predecessors. They also require Plavix, but only for 3-6 months.
As stents have improved, so have statistics regarding cardiovascular disease. We see fewer heart attacks, strokes, and sudden cardiac death as a result of aggressive lipid management and appropriate use of stenting for acute chest pain. Overall, things in the cardiovascular disease area have changed for the better, and there’s nothing out there to say it won’t continue to improve. No longer is angina pectoris, chest pain due to CAD, just “sat on.” Nitroglycerin tablets aren’t prescribed with the frequency they were 20+ years ago, because when a patient has angina, they get cathed and stented or have a coronary bypass procedure. No longer are patients “watched” or “observed.” Those folks have a bad habit of dropping dead, and cardiologists like to keep that from happening. Aggressive cholesterol management plus stenting are the means to prevent those problems.
So, yes, changes are coming, but many are already here!
References: Riera E., Trial Data May Shift Coronary Artery Disease Treatment. medscape.com 2026 April 22.
www.google.com/search?q=what+are+first+generation-stents
www.google.com/search?q=what+are+second+generation+stents

