-ITIS and -OSIS: WHICH IS WHICH?

Medical terminology is often confusing. Beside the fact that many terms have multiple syllables and a lot of letters, they have defining endings like -ology, -itis, -osis, -oid, and -oma that clarify the specific meaning. This can be very problematic for folks who didn’t take a course in Greek and Latin derivatives in high school or college, but when one learns the meaning of these suffixes, it’s much easier to understand what’s being said and how to respond to it.
One of those confusing misunderstandings is the difference between diverticulosis and diverticulitis. Very often I’ve heard patients and the public express uncertainty about the meaning of each term. They will use diverticulosis when they mean diverticulitis and vice versa. It becomes even more confusing when one considers the singular and plural forms of the word-diverticulum and diverticula. Then, confusion increases when one considers, for example, gender differences such as alumnus (male singular) and alumni (male plural). Add to the gender difference alumna (female singular) and alumnae (female plural). Fortunately, inanimate objects, like diverticula, have no gender specificity, and are usually given the male designation. But although it’s not in the dictionary, doctors use diverticuli interchangeably with diverticula.
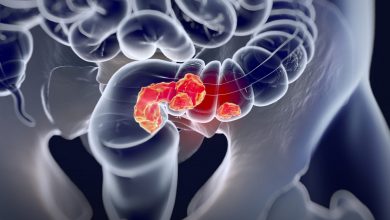
So, what’s the difference? Diverticula (the plural of diverticulum) are out-pouchings in the wall of the gastrointestinal tract, most frequently in the lower colon, caused by weakness in the muscular layer of the colon wall. Diets low in fiber and high in animal fat, chronic constipation, and family history play a large role in the development of diverticula.
Diverticulosis is defined as the presence of diverticula in the colon. It just means you have these small pockets in the colon wall. On the other hand, Diverticulitis means the person’s diverticula have become inflamed and infected. Diverticula are asymptomatic except when accompanied by constipation, but when they become infected, pain, abdominal tenderness, and fever occur. So, diverticulosis is a condition that is usually benign and not accompanied by illness, and diverticulitis is an acute infection of the colon accompanied by significant symptoms.
Diverticulosis has always been considered a disease of the elderly. It is present in 10% of the population over age 40, 50% of patients over age 60, and virtually everyone over the age of 80. It’s also regarded as a disease of “Western civilization” occurring far more often in the United States, Europe, and Australia than in Africa and Asia. “The Western diet, low in dietary fiber, has long been implicated as a causative factor for these geographical variations.” “Dietary fiber intake has been found to be inversely associated with the risk of developing diverticulosis.” The higher the fiber content in one’s diet, the lower the incidence of diverticulosis.
Additionally, diverticulosis in western countries is primarily left-sided, involving the sigmoid colon (the last section of colon before the rectum). This is in contrast to Asian countries where right-sided diverticulosis predominates. The reason for this difference is unknown, but factors other than dietary fiber are probably responsible for the difference.
About 20% of patients with diverticulosis have complications, one of which is diverticulitis. Food particles and bacteria clog the diverticula and eventually cause infection. About 25% of patients with diverticulitis have further complications such as abscesses, fistula formation, obstruction, and perforation. Perforation leads to spilling of fecal material into the abdominal cavity and peritonitis, a serious and emergent complication. Recurrent episodes of diverticulitis are common and cause scarring (fibrous structuring) of the colon, resulting in obstruction.
Treatment of diverticulitis in uncomplicated cases is usually outpatient oral antibiotics. More severe cases require hospitalization and intravenous antibiotics. Surgical excision of the diseased segment of bowel is recommended for recurrent episodes or for any complicated cases. Most often, removing the diseased segment is curative unless, of course, the extent of involvement is widespread. For those cases complicated by perforation and peritonitis, surgery is done emergently, the perforated segment is removed, the healthy colon is diverted to a temporary colostomy, and the remaining colon beyond the perforated section is closed off and left to rest and heal. After several weeks, or months, the colostomy is “taken down” (removed) and the colon and end segment reattached (re-anastomosed).
It used to be thought that patient’s with diverticulosis should avoid eating nuts, seeds, shells, etc. due to concern they would trigger infection, but that thinking had been refuted. But it is well-accepted that a low animal fat, high fiber diet will act as a preventive for the development of diverticula.
Dr. G’s Opinion: I saw one or two patients a month with acute diverticulitis. It is easily diagnosed by history, physical exam, and CT of the abdomen and pelvis. Radiologists are very skilled at detecting inflammation, abscess formation, and even small, sealed-off perforations of the colon. The majority of patients got better after a course of oral antibiotics. But since the diverticula were still there, they were likely to flare up again unless the patient made a drastic change in his/her dietary habits. That rarely happened. Most patients who had recurrent diverticulitis didn’t have surgery until some complication arose. Elective colon resection would be ideal, but regrettably, most patients put it off. One question I asked every diverticuliitis patient was “Do you eat a lot of popcorn?” I was amazed how frequently the answer was,”Yes, I eat popcorn several times a week.” I’m sure there’s a study out there somewhere correlating popcorn intake to diverticuliitis, but I haven’t seen it. In another post there is a list of foods patients should avoid if they have diverticulosis. Check it out if you’re interested.
So cut out the animal fat, increase the fiber in your diet, drink fluids, and try to be “regular.”
References:
“Diverticular Disease: Epidemiology and management,” Weizmann and Nguyen. Can J Gastro-
enterology, Vol 25, No 7, July 2011.
MedlinePlus.gov/diverticulosis and diverticulitis
ClevelandClinic.org/diverticulosis-diverticulitis