Acute ankle injuries are very common. It’s a rare athlete who hasn’t sprained one our both ankles at sometime during their sporting life. Sprains occur as a result of forced movement of the ankle that exceeds the ligaments ability to maintain the structural integrity of the ankle joint. The force causes the foot to move inward spraining the lateral (outer) ligaments of the ankle. If the foot is forced outward (laterally), the ligaments on the inside of the ankle are sprained. Ligaments are sprained. Muscles are strained.
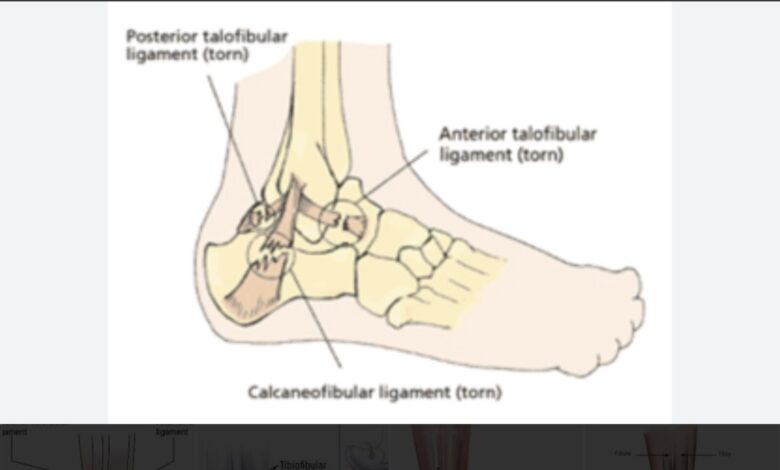
The bones of the ankle are not involved in sprains. The talus, calcaneus, and tibia and fibula form the bony structure of the ankle joint. There are three major ligaments that hold the bones together to maintain the joint and permit us to walk, run, and jump.
In lateral ankle sprains, the most common type of sprain, the anterior talofibular ligament (AFL) is torn. That ligament connects the talus to the fibula. In more severe lateral ankle injuries, the deltoid ligament is also torn.
In medial ankle sprains, the medial ligament is the injured part. A more recently discovered injury is the high ankle sprain. The tibia and fibula form the inside (medial) and outside (lateral) margins of the ankle. The two bones are held together by a ligament that connects the inside and outside bones at the ankle.
Ankle sprains are graded by severity as grades I, II, and III. Unfortunately, the only way these can be accurately determined is by direct observation or by MRI, but grading is purely academic and isn’t used to decide on treatment. Grade I is a microscopic ligament tear, Grade II is a partial tear, and Grade III is a complete tear.
The obvious signs of ligament damage to an ankle are pain, swelling about the malleoli, collections of blood under the skin, and increased pain with weight bearing. If you’ve ever had a sprained ankle you’re very familiar with the symptoms.
Treatment is based strongly on “protecting the joint,” meaning immobilization by splinting while also attempting to maintain functional motion by exercises. Limited weight bearing, initially, is protective as well. Icing the joint as soon as possible helps keep swelling at a minimum. Pain control is accomplished by reducing swelling through elevation and icing in addition to oral analgesics like acetaminophen, ibuprofen, or hydrocodone if pain is not otherwise controlled. Later, weight bearing and gentle exercise are advised while continuing immobilization.
After the acute pain subsides, rehabilitation exercises with bracing enable the patient to gradually return to normal activities and regain full function. Bracing should be continuous for 4-6 weeks followed by the use of removable external supports during sports activities for up to 12 months depending on the individual’s progress and degree of pain. Restoring range of motion is the goal of rehab and control of swelling and exercises to increase range of motion are recommended. Returning to sports activities can take 8 to 12 weeks and should not be rushed along unless you’re the franchise athlete who carries the team.
If pain and disability persist an unreasonable length of time, an occult (hidden) fracture should be looked for. Fractures of the talus bone, cartilage injury, or peroneal tendon problems can cause persistent pain.
Acute ankle sprain is a very common problem. If not treated properly, it can result in a painful, chronically swollen, unstable ankle. Surgery for torn ankle ligaments is rarely, if ever, done. Once an ankle sprain has occurred, the likelihood for repeat injury is very high. “Rolling” an ankle can happen so easily with very little force. Athletes have to strengthen the muscles around the ankle to prevent recurrent sprain. Fortunately, ankles do get better and usually don’t cause long term problems.
References: Wu V, Padilla CA, Smith NA. Management of Acute Ankle Sprains: Common Questions and Answers. Am Fam Phys 2025 Dec;112(6):609-617.
Kerhoffs GM, et al. Diagnosis, treatment, and prevention of ankle sprains: an evidence-based clinical guideline. Br J Sports Med 2012;46:854-860.