The first thing important for this blogpost is an understanding of fibromyalgia. This disorder is fairly common, but often is not given the name, fibromyalgia. It’s a chronic pain syndrome in which, more commonly women (3:1 over men), have widespread pain that varies in location and severity. It is characterized by tenderness of at least 11 of the 18 identified trigger points paired on the body. These trigger points are tender to touch and the number of points involved vary day to day. To be diagnosed as fibromyalgia, 11 of the 18 trigger points must be tender, and must be for 3 months or longer.
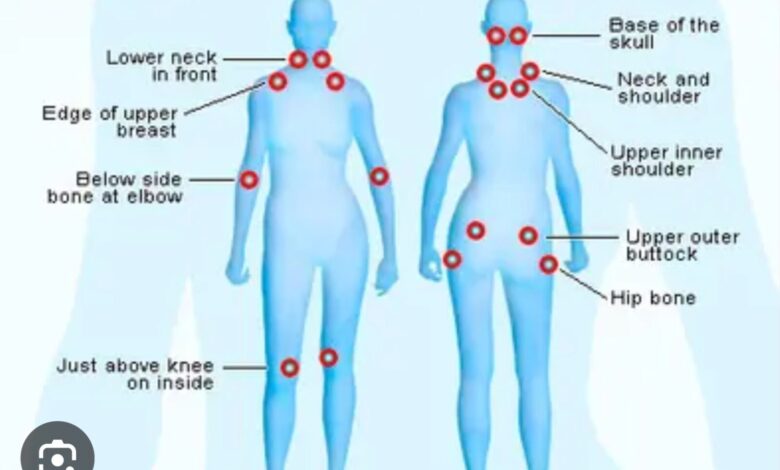
Trigger points are found:
At the base of the back of the neck
Between the shoulder and neck
At the junction of the collar bone and breast bone
At the junction of the ribs and breast bone
At the outer aspect of the elbows — the lateral epicondyle
At the outer aspect of the hips — the greater trochanter
The sacroiliac joints
At the inner aspect of the knees
Fibromyalgia patients also have problems sleeping, bowel difficulties, mood swings, and headaches. Anxiety and depression are prominent symptoms seen in fibromyalgia.
Treatment of fibromyalgia can be difficult and success is often only partial relief of pain. It is a chronic disorder for which there is no cure and symptoms are merely controlled or moderated, not eliminated. All sorts of drugs and combinations of drugs have been tried to control fibromyalgia. There is limited to no evidence that narcotics (oxycodone, hydrocodone, morphine, Dilaudid, and cannabinoids) provide any relief. In fact, narcotics are certain to foster dependence which actually worsens the situation. NSAID’S have too many adverse effects to justify the very minimal benefit they have in fibromyalgia. Antipsychotics, anticonvulsants, and tranquilizers have been prescribed, but are ineffective.
The combination that has been used successfully for the past 15+ years includes Pregabalin (Lyrica), duloxetine (Cymbalta), and milnacipran (Savella) in various dosages and combinations.
Lyrica (pregabalin) is the cornerstone/root of fibromyalgia treatment. Technically, it is classed as anticonvulsant, but is rarely prescribed for that reason. Instead, it is very effective against chronic pain syndromes such as exist in fibromyalgia. To complement Lyrica, duloxetine is the drug of choice. It is a combined SSRI (selective serotonin reuptake inhibitor–like Prozac ) and SNRI (selective norepinephrine reuptake inhibitor) that relieves pain by its effect on neurotransmitters. If the Lyrica-Cymbalta combination fails, Savella replaces Cymbalta. Savella has the same profile as Cymbalta but has a higher potency and is more effective.
The duloxetine-pregabalin combo is used as an everyday treatment to suppress pain, but when trigger points flare, local trigger point injections with corticosteroid and anesthetic are temporarily helpful.
There are a lot of folks “out there” who suffer with fibromyalgia but are undiagnosed or are misdiagnosed. The duloxetine-pregabalin combination has been effective for over a decade and has just been validated by Cochrane reviews. Cochrane in an independent, global, medical review organization that consolidates research on medical topics then issues their opinions, evaluations, and criticisms. Their publications are widely respected.
So, if you’re a known fibromyalgia sufferer, or if you are suspected of having it, you now have helpful information to arm yourself when you see your physician.
References: POEMs: Patients-Oriented Evidence That Matters; “Good Evidence that Duloxetine, Milnacipran, and Pregabalin Provide Meaningful Pain Reduction in Adults with Fibromyalgia. Am Fam Phys 2025 October;112(4):456.
Moore A, Bidonde J, Fisher E, et al. Effectiveness of pharmacological therapies for fibromyalgia syndrome in Adults: An Overview of Cochrane Reviews Rheumatology (Oxford) 2025 May



