CANCER is a word no one wants to hear, especially if it’s associated with your name. It’s probably the most feared diagnosis people can receive because it carries with it uncertainty, anxiety, and the fear of death. When you hear someone has cancer, your first emotions are sadness because they have it and compassion because you know they are probably going to have to endure surgery, chemotherapy, and/or radiation therapy plus they just might die. You really don’t want that to happen to anyone. We’ve all heard horror stories about the misery and suffering people with cancer are subjected to, and that’s not what you want for your friend or loved one. You bargain with God, ask for prayers from everyone, research treatments, and try to find the best doctor(s) you can. You want to employ every resource you can to improve your chances of a cure.
This is all meant to serve as an introduction to an explanation of cancer: What is it? What terms describe and classify it? How does it affect healthy people? Why are some cancers worse than others? What happens to cause death?
Cancer is defined as the abnormal growth and multiplication of the cells of the involved organ or tissue. Due to various factors, the genetic make-up the involved cells is altered (mutates) causing the cells to grow and multiply in an abnormal, uncontrolled manner. These “cancer” cells push normal cells aside and replace them with abnormal cells that starve normal cells of their nutrients and cause them to shrink and die. Cancer cells invade and disrupt blood vessels and damage the lymph channels that drain tissues of their waste products. The involved organ/tissue ceases to function properly, and the patient experiences some of the many symptoms that cancer can cause.
Many terms are used to classify cancer and an explanation of these is worth pursuing.
Cancer is a form of neoplasia which means new formation or new growth. So a neoplasm is a new growth of tissue within an existing normal tissue. There are benign and malignant neoplasms. A benign neoplasm is one in which the new growth is confined to a single mass surrounded by a distinct margin and the cell growth and division is slow. In a malignant neoplasm, cell growth and multiplication are very rapid, the cells have a significantly abnormal appearance microscopically, and the margins are indistinct. The difference is determined by a pathologist, a physician who examines tissue biopsy samples under a microscope.
“Oma” is a suffix that means swelling or tumor, and is added to other terms to identify the location or type of the tumor. Examples are carcinoma, sarcoma, fibroma, myeloma, neuroma, glioma, etc. A tumor is a very non-specific term that can refer to any lump, bump, or growth anywhere on the body and does not refer only to cancer. Tumor and cancer are not synonymous.
Cells don’t just suddenly become cancerous. They undergo a slow transition from normal to cancer. In other words, over time, the characteristics of the cells gradually change. These phases are described microscopically as follows:
Normal: no abnormal cellular appearance microscopically
Hyperplasia: a marked increase in the number of normal cells in a tissue/organ
Dysplasia: abnormal appearing cells microscopically but no characteristics of cancer
Cancer: microscopic evidence of malignant cells in biopsy
Examples of the above are “benign prostatic hyperplasia,” the term given to an enlarged, but non-cancerous, prostate, and “cervical dysplasia,” a pre-malignant change found on PAP smear or biopsy of the uterine cervix.
Other terms are determined by the tissue or organ from which the cancer cells originate.
Carcinomas originate from epithelial (outer surface) or glandular tissues.
Sarcomas originate from connective tissue, muscle, nerve, or endothelial (inner surface)
tissues.
Carcinomas can be Adenocarcinomas, Squamous Cell Carcinomas, or Basal Cell Carcinomas.
Adenocarcinomas begin in cells that produce fluids or mucus. Examples are breast, colon, and prostate cancer, but many others exist as well.
Squamous Cell Carcinomas originate from cells of the outer surface layers such as the skin,
stomach, intestine, lungs, bronchial tubes, bladder, and kidney. Another term for squamous carcinoma is “epidermoid” carcinoma of whatever organ is involved.
Basal Cell Carcinomas originate from the basal cell layer of the skin and exist only as a type of skin cancer.
Transitional Cell Carcinomas originate from the transitional cell layer of the surface of the urinary bladder, the ureters, or the kidneys.
Sarcomas develop in bone or soft tissues and carry the name of the tissue of origin. Examples are Osteosarcoma (bone cancer), Chondrosarcoma (cancer of the cartilage), and Myosarcoma (cancer of a muscle).
Leukemias are cancers of the blood-forming tissues of the bone marrow. The type of white blood cell involved is included in the name. Examples are Lymphocytic leukemia (cancer of the lymphocyte WBC’s) and Myeloid leukemia (cancer of the neutrophil WBC’s). Leukemias can be acute or chronic determined by the microscopic characteristics seen by the pathologist.
Lymphomas are cancers of the lymph nodes and lymphatic channels. Two main types exist: Non-Hodgkins and Hodgkins Lymphomas. These are determined by the microscopic appearance of the biopsy specimen.
Multiple Myeloma is a cancer of the plasma cells of the bone marrow. It destroys the bone marrow and invades bone. It is also called Plasma Cell Myeloma or Plasmacytosis.
Melanoma originates from the melanocytes (pigment-producing cells) of the skin.
Brain and Spinal Cord cancers are named for the type of cell involved such as astrocytes or astrocytoma.
Germ Cell, Neuroendocrine, and Carcinoid tumors are rare forms of cancer that develop from specialized cells in various areas of the body.
As mentioned previously, genetic mutations of cellular DNA change the growth and multiplication patterns of cells resulting in rapid growth and division that cannot be controlled. These changes can occur before birth (are inherited) or occur after birth due to external factors, listed below. When cancer is genetically inherited, 50% of inheriting offspring will acquire the gene, but for unknown reasons many of those patients will never have clinical evidence of cancer. Over time, however, the risk of developing cancer increases significantly.
Besides the genetic inheritance of cancer genes, external factors can cause cancer as well. Viruses such as Human Papilloma Virus (HPV) and Hepatitis B and C viruses are known to cause cancer of the cervix and liver. Epstein-Barr virus disease and Kaposi’s sarcoma are other examples. Bacteria such as Helicobacter pylori are associated with B-cell lymphoma of the stomach. Environmental factors such as tobacco, diet, air pollution, alcohol abuse, asbestos, industrial pollutants, ultraviolet radiation, and hormones all have significant roles in causing various cancers. These factors have an ever-increasing relevance in our society and in the occurrence of cancer.
Malignant cancers metastasize. That means by several mechanisms, cancer cells spread to other tissues or organs. They spread locally (in their current location) by growing larger, damaging the nearby normal tissue. Then, as the tumor enlarges, cancer cells mechanically invade adjacent tissues, organs, blood vessels, or lymph channels. When cancer cells invade blood vessels (hematogenous dissemination) and lymphatic channels (lymphogenous dissemination), they are transported to other areas of the body causing metastatic lesions (tumor growths) to develop in the tissues or organs where they end up.The presence of “Distant metastases” is a very bad prognostic factor. The lungs, liver, brain, and bones are common sites of distant metastases.
Because cancer is such a complex disorder, to establish consistency among treating physicians, to understand the severity of the individual disease, and to determine prognosis, cancer staging criteria have been developed. Every type of cancer has its own set of staging criteria, but the basic criteria have two classifications. These are Staging Criteria and TNM Classification. These “stages” are determined by the pathologist and oncologist. In addition, the pathologist’s microscopic examination determines the “grade,” or degree, of malignancy of the specimen from its histologic appearance. Grade is also called “Differentiation.” The more differentiated the specimen is the less malignant it is. So a well-differentiated biopsy specimen has low malignant potential while a poorly differentiated, or undifferentiated specimen is highly malignant. The numbers 1-4 are used to grade malignancy, but more commonly the term differentiation is used. It is cellular “differentiation” that is responsible for some cancers progressing more rapidly than others from the same organ or tissue.
The oncologist or cancer surgeon determines the TNM and Staging criteria. Stage criteria are:
Stage 0 is Carcinoma in situ-abnormal looking, pre-cancerous cells on the surface layer of the involved tissue without local extension.
Stage 1 cancer is confined to site of origin
Stage 2 cancer has spread within the site of origin-local extension
Stage 3 cancer has spread to adjacent tissues outside of site of origin or to regional lymph
nodes-local metastases.
Stage 4 cancer has spread to distant organs (lungs, liver, brain, etc.)-distant metastases.
TNM Criteria are far more complex, and numerous subclassifications exist. Basic understanding of the system is as follows:
T stands for Tumor. It designates the origin and size of the cancer. (TX, T0, T1,2,3,4)
N stands for Nodes and which ones and how many are invaded by cancer cells (NX, N0,
N1,2,3)
M stands for Metastases the presence or absence thereof. (MX, M0, M1)
As mentioned, each criterion is numbered based on criteria determined by surgery or imaging studies like PET scanning, CT scans, or MRI scans. An example of TNM staging would be T1N2M1 which means a small sized tumor has spread to a few nodes and to distant organs. Any lymph node involvement or distant metastasis carries a poor prognosis. This complicated classification may change due to changing circumstances in the patient. Patients are re-staged during each visit and after imaging results are obtained. So the score could change to T3N3M1, for example.
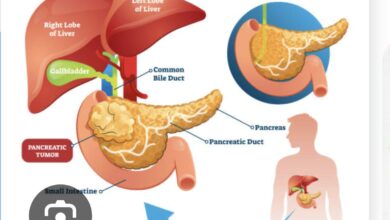
I hope this explanation and defining of cancer terms is of help to you. I also hope these terms are never associated with you or your loved ones. Cancer treatment has improved in recent decades and cure rates for many cancers have improved greatly. But breast, lung, pancreatic, brain, and ovarian cancers, and multiple myeloma and melanoma are still worrisome diagnoses. These cancers are particularly adept at defying early detection or have a propensity for recurrence and thus have poor prognoses. The best one can do is take advantage of every screening opportunity available and don’t fail to see your doctor on a regular basis.
The diagnosis of Cancer doesn’t have to be a death sentence, but unfortunately, it still has the potential to cause significant morbidity (unhealthy life) and mortality (death). We can only hope researchers find the treatment that reverses the factors causing cancer.
References: Neoplasia AState.edu
healthline.com/malignant neoplasms


купить защиту диплома <a href=[Link deleted].
Thank you.
Thanks for some other great article. The place else could anyone
get that type of info in such an ideal way of writing?
I’ve a presentation subsequent week, and I’m at the look for
such info.
My web page :: <a href="[Link deleted]
Thank you.
content i find it hard to identify really good facts out there when it comes to this topic appreciate for the blog post
Thanks